
Hip Physiotherapy
Spesific conditions
Primary function of the hip joint
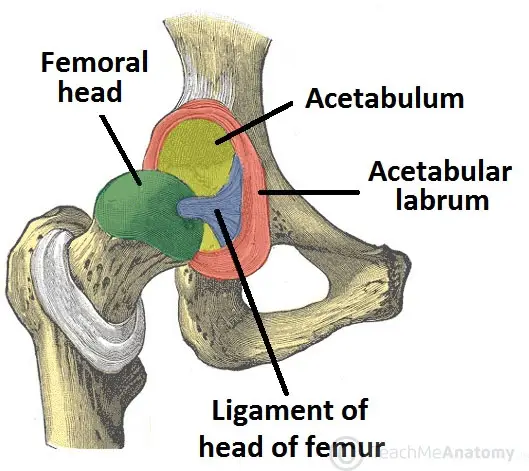
Anatomy, Injuries, & Symptoms of the hip
FEMOROACETABULAR IMPINGEMENT (FAI)
PINCER
Cam leasion
CAM LESION

Laberal tears
LABRAL TEARS
Chondropathy
Hip flexor
HIP FLEXOR INJURIES
Iliospoas bursitis
ILIOSPOAS BURSITIS
Injury symptoms
Inguinal hernias
INGUINAL HERNIAS

DIRECT HERNIA
INDIRECT HERNIA
Hernias are not usually life-threatening; however, they can become so if the hernia becomes strangulated.
Greater Trochanter pain syndrom (GTPS)
GREATER TROCHANTER PAIN SYNDROME (GTPS)

What is the cause of gtps pain?
How is gtps treated?
Muscular issues and imbalances around the hip
MUSCULAR ISSUES AND IMBALANCES AROUND THE HIP
The ligaments & muscles
THE LIGAMENTS
THE MUSCLES
HIP ADDUCTION
The muscles that adduct (bring the leg towards the body), are known as the adductor group of muscles and consist of the following : anteriorly; the adductor magnus, longus and brevis, gracilis and pectineus; posteriorly; the obturator internus and externus.
HIP FLEXION
The iliopsoas (made up of the iliacus and psoas major and minor muscles) is the major flexor of the hip joint. Along with the Sartorius, rectus femoris and tensor fascia latae (TFL) muscles, the iliopsoas allows bending at the hip. The Sartorius muscle is also responsible for moving the limb up and outwards (abduction and external rotation).
HIP ABDUCTION
The two muscles that serve to abduct or move the lower limb away from the body are the gluteus medius and minimus. These muscles are located on the outside of the hip and are essential for maintaining pelvic stability. This is by the presence of a ‘Trendelenburg’ gait. This occurs when the gluteus medius muscle is weak on the weight bearing side and hence causes the pelvis to sag on the opposite side.
HIP EXTENSION
The muscles at the back of the hip function to extend, externally rotate (rotate outwards) and adduct (bring towards the body) the hip. The muscle action varies based on the attachments and fibre directions, and several muscles have dual functions. For example, the Gluteus maximus, which is the largest muscle of the group, serves to extend and externally rotate the hip. The piriformis muscle is a much smaller muscle with similar functions. Other muscles at the back of the hip include the gemelli superior and inferior, the obturator internus and externus, and quadratus femoris.
How do the muscles of the hip provide protection?

Primary function of the Hip Joint
Anatomy, Injuries & Symptoms of the Hip

Femoroacetabular Impingement (FAI)
Pincer
Cam Lesion
Labral Tears
Chondropathy
Hip Flexor Injuries
Iliospoas Bursitis
Iliospoas Bursitis injurie symptoms
Inguinal Hernias
Direct Hernia
Indirect Hernia
Hernias are not usually life-threatening; however, they can become so if the hernia becomes strangulated.
Greater Trochanter Pain Syndrome (GTPS)
What is the cause of GTPS pain?
How is GTPS treated?
Muscular Issues and Imbalances Around the Hip
The Ligaments
The muscles
HIP ADDUCTION
The muscles that adduct (bring the leg towards the body), are known as the adductor group of muscles and consist of the following : anteriorly; the adductor magnus, longus and brevis, gracilis and pectineus; posteriorly; the obturator internus and externus.
HIP FLEXION
The iliopsoas (made up of the iliacus and psoas major and minor muscles) is the major flexor of the hip joint. Along with the Sartorius, rectus femoris and tensor fascia latae (TFL) muscles, the iliopsoas allows bending at the hip. The Sartorius muscle is also responsible for moving the limb up and outwards (abduction and external rotation).
HIP ABDUCTION
The two muscles that serve to abduct or move the lower limb away from the body are the gluteus medius and minimus. These muscles are located on the outside of the hip and are essential for maintaining pelvic stability. This is by the presence of a ‘Trendelenburg’ gait. This occurs when the gluteus medius muscle is weak on the weight bearing side and hence causes the pelvis to sag on the opposite side.
HIP EXTENSION
The muscles at the back of the hip function to extend, externally rotate (rotate outwards) and adduct (bring towards the body) the hip. The muscle action varies based on the attachments and fibre directions, and several muscles have dual functions. For example, the Gluteus maximus, which is the largest muscle of the group, serves to extend and externally rotate the hip. The piriformis muscle is a much smaller muscle with similar functions. Other muscles at the back of the hip include the gemelli superior and inferior, the obturator internus and externus, and quadratus femoris.
How do the muscles of the hip provide protection?
Injury avoidance & recovery for hip injuries
